Clinical Development Strategy In Rare Diseases

Clinical trials in rare diseases present more significant challenges compared to trials in more common diseases. These challenges arise due to various factors, including trial design, the limited patient population for recruitment, regulatory support, and more. However, implementing a well-defined strategy for clinical development in rare diseases can help overcome these challenges. Such a strategy has the potential to expedite the drug development process for orphan diseases.

Every step involved in the development shall be considered precisely and planned strategically. This helps to overcome all the challenges that arise in the clinical development process, which include
- Choosing a modern adaptive trial design,
- Conducting country-level feasibility even before initiating any clinical trial,
- Considering the regulatory scenario (the incentives offered by the regulator which boost the development process),
- Choosing the right qualified sites and clinical investigators,
- Considering other factors such as site reachability, virtual patient monitoring
If the trial design imposes a disproportionate burden of participation, recruitment may fail or participants may drop out before trial completion. Avoiding unnecessary designs and considering adaptive trial designs is a strategy that may improve patient participation.
When maximizing the chance of a successful trial, involving patients or parents of a child with a rare or ultra-rare disease in the early stages can play a pivotal role. This is particularly important as most rare diseases occur in the pediatric population.
Before moving into further details, let’s look at the statistics of rare diseases
Rare Disease Statistics
- 3.5 to 5.9% of the global population suffers from rare disease conditions.
- The Global Genes Project estimates that around 300 million people are affected by a rare disease, which is about 4% of the world population.
- More than 6,000 diseases are listed on the Orphanet, of which 72% are genetic, and 70% start in childhood. Among these diseases, 149 alone are responsible for 80% of cases of rare diseases identified worldwide.
Globally, there are a total of 2,225 clinical trials on rare diseases. The major number of studies take place in North America, followed by Europe and East Asia.
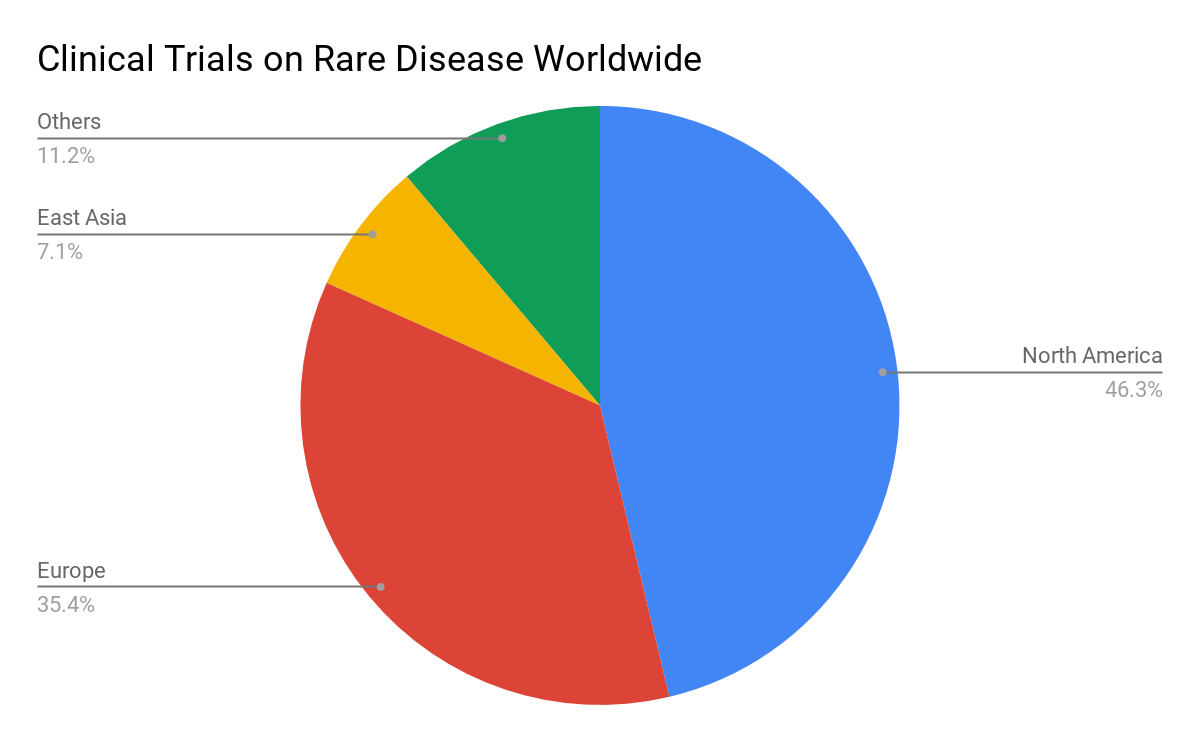
From the statistics above, it’s evident that clinical trials in rare diseases are predominantly conducted in developed regions such as the USA, Europe, Japan, etc. This preference can be attributed to the following reasons.
- The strong and a clear regulatory pathway
- Prevalence of disease and availability of patients for recruitment
- Clinical trial awareness among patients
- Regulatory support for conducting clinical trials in rare diseases, such as providing acceleration in the approval process, incentives, etc.
How clinical development strategy is different from other trial strategies
Global regulatory
- The development of treatments and drugs for rare diseases is financially not viable and is more prominent in very rare diseases. Hence most companies require support from the regulations in the matter of gaining faster approvals, financial benefits, and early access to the market.
- Regulators of developed countries like the USA, EU, Australia, and Japan offer good benefits and incentives to push the rare disease drug developers and to foresee the best treatments available for unmet diseases.
- Now even the regulators of countries like Russia, China, South Korea, India, etc. are working on improvements in regulations for providing benefits for orphan disease drug developers.
Please look at our previous articles about various incentives provided by regulators for rare disease drug development in the USA, Europe, Australia, Japan and other Asean countries
Country selection for your rare disease
Choosing the right region for your rare disease clinical trial is crucial and greatly influences the likelihood of success. Conducting country-level feasibility can help achieve this. It involves assessing factors such as trial completion timelines, disease prevalence, the patient population for recruitment, qualified sites and investigators, and more.
Clinical trial design and Evaluation
The clinical trial design plays a crucial role in determining several aspects. This involves several factors. It includes the number of patients required to be recruited for a study. Additionally, it encompasses the data that need to be generated in compliance with regulatory requirements. Lastly, it considers the minimum number of patients.
- An important factor in the rare disease is that not all patients present with the same disease subtypes, and this makes recruitment more difficult.
- Choosing adaptive trial designs, designs that involve infrequent patient visits, and minimum resources may be one of the strategies. Trial designs must be simplified, flexible, and attractive to enroll enough patients.
- Choosing a trial design such as a platform, bucket, or umbrella shoots more flexibility and with few resources, yet extracting quality data.
- The US FDA also recommends using such trial designs and provides guidance documents for such trials. Rare disease patient populations are often heterogeneous in disease subtypes.
Here are some examples of using new trial designs for a better approach and adaptability.
Example 1
The BRAF-V600 study is a trial comprising multiple sub-studies. Its purpose is to evaluate the efficacy of vemurafenib for non-melanoma BRAF V600E mutation-positive cancers. Hyman et al., Cunanan et al., and Woodcock and LaVange all classified this study as a basket trial. The Simon two-stage design determines the sample size for each sub-study.
Example 2
The FOCUS4 trial is evaluating the efficacy of multiple targeted therapies for untreated colorectal cancer. It is being conducted through a placebo-controlled, multi-group, multi-stage randomized trial. In stage 1, the researchers evaluate the safety, and in stage 2, they confirm proof of concept. Stage 3 assesses short-term outcomes, while stage 4 evaluates long-term efficacy in a patient population with a particular molecular marker.
The categorization of the FOCUS4 trial is as an umbrella trial, which can also be classified as a platform trial.
Click here to know about RCT, Adaptive, Umbrella, Basket and Platform trial designs
Patient recruitment and retention
Patient recruitment and retention are another consideration in the clinical industry, as most of the trials fail in successfully recruit patients and retaining them and prolonging the trial duration to many years.
It is mainly due to a lack of proper strategic planning and execution. Patient recruitment is a point of concern even before designing a trial as the trial design determines the number of patients and the type of patients required for a clinical trial.
- Part of the strategy for patient recruitment involves selecting a country. Developed countries like the USA and Europe offer numerous access points for patient recruitment. These include applications, organizational databases, websites, and various portals that provide information on rare disease patients.
- Another solution to this challenge is to use real-time patient data and physicians’ notes from electronic health records (EHRs) to model various recruitment scenarios,
In general, when designing a clinical trial for rare diseases, it is important to consider the geographic scattering of patients. Factors such as the frequency of patient visits to sites, travel incentives, and direct-to-patient (DTP) methods should be taken into consideration.
Producing quality clinical trial data
Utilizing designs that require minimum resources yet yield efficient and quality data is often challenging and can be defined in strategic planning.
- Measuring clinical trial outcomes, especially in rare disease patients, is challenging as they often exhibit diversity in their clinical presentation and histories.
- Reported outcomes, whether clinician-reported, observer-reported, or patient-reported outcomes (PROs), are influenced by variables such as age, disease progression, and disease severity.
- Regulators like EMA, and US FDA, recommend utilizing efficient trial designs that yield quality data within minimum patient fetching for rare disease developers.
- FDA offers guidance documents for such adaptive trial designs more frequently used in cancer rare disease trials.
Are you looking for support in your drug development for rare diseases?
Talk to us today. Provide details of your requirements and we will connect with you.