Functional Service Provider (FSP) in Clinical Trials: What the Model Is, When It Works, and What Sponsors Often Get Wrong
The Functional Service Provider (FSP) model gives sponsors something that full-service CROs and pure in-house execution don’t: operational depth in specific markets or functions, without surrendering governance of the study. When sponsors use it well, they get experienced on-ground staff, maintain data and IP control, and run leaner than a full-service model allows. When they use it poorly, they add a layer of external resource without the internal structure to direct it.

This article covers what FSP is, how it compares to the alternatives, when it works and when it doesn’t, what the best FSP relationships look like in practice, and what sponsors most commonly get wrong.
Key takeaways
- FSP places CRO staff into your study under your governance: the sponsor retains strategic ownership, and the provider supplies and manages the people.
- The model works best when you already have functioning SOPs, systems, and a capable sponsor-side project manager. It is not a substitute for those things.
- FSP is a governance and continuity model, not a cost-reduction strategy in isolation. Cost savings follow from the model working correctly, not from choosing it before the preconditions are in place.
- In APAC, local language fluency and market-specific regulatory knowledge are the most important capabilities to verify in any FSP provider.
- When FSP works well, sponsors consistently report faster site activation, stronger investigator relationships, better data quality, and 20 to 35% cost savings versus equivalent full-service APAC arrangements.
- The most common failure mode is a sponsor nominating a project manager who lacks the capacity or authority to actually direct the FSP staff.
What FSP actually means
FSP stands for Functional Service Provider. In a clinical trial context, it means a CRO provides staff and specific functional capabilities on a resource-provision basis, within the sponsor’s own governance structure. The sponsor retains strategic ownership of the study. The CRO supplies the people.
In practice:
- The sponsor provides the SOPs, the study protocol, and the systems (EDC, CTMS, eTMF, safety database).
- The FSP provider places staff (typically CRAs, clinical trial managers, data managers, or clinical monitors) into the study.
- Those staff work to the sponsor’s SOPs, file into the sponsor’s eTMF, and report to the sponsor’s project manager.
- The CRO is responsible for personnel quality, onboarding, backfill, and HR. The sponsor is responsible for directing the work.
This is distinct from staff augmentation, where individual contractors are placed directly with the sponsor on a time-and-materials basis with no CRO layer. In FSP, the provider retains employer accountability. It is also different from full-service, where the CRO assumes end-to-end project management under its own SOPs.
The diagram below shows how responsibilities are divided between the sponsor and the FSP provider. The sponsor retains strategic ownership of the study at every stage; the FSP provider supplies and manages the clinical staff who execute it on the ground.
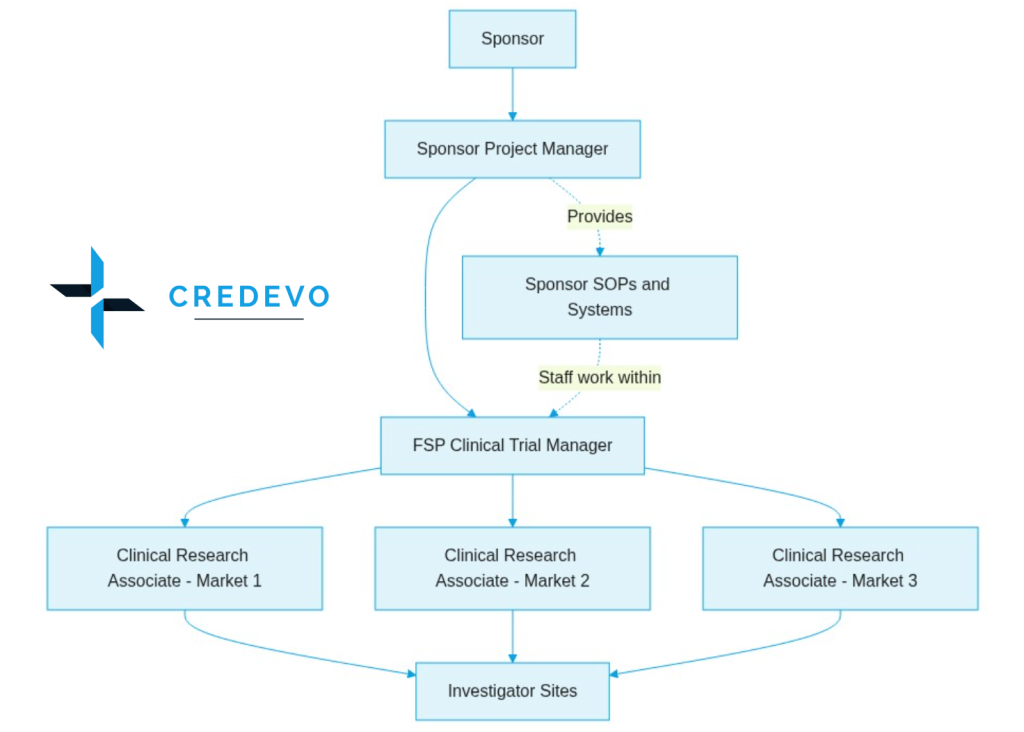
Figure 1: FSP governance structure.
Solid lines show the direction of authority from the sponsor down to the sites. Dotted lines show that FSP clinical staff work within the sponsor’s own SOPs and systems throughout the study. SOPs: Standard Operating Procedures; eTMF: Electronic Trial Master File; EDC: Electronic Data Capture.
FSP, full-service, and standalone: what each model does
Understanding FSP requires clarity on what the alternatives offer and where the governance boundaries sit.
| Dimension | Full-service CRO | FSP | Standalone (in-house) |
|---|---|---|---|
| Who manages the study | CRO project manager | Sponsor project manager | Sponsor team |
| Whose SOPs apply | CRO SOPs | Sponsor SOPs | Sponsor SOPs |
| Who owns the eTMF | CRO (typically) | Sponsor | Sponsor |
| Who owns data governance | Shared or CRO-led | Sponsor | Sponsor |
| Best-fit sponsor profile | Limited internal clinical ops, or entering a new region for the first time | Functioning internal team that needs regional execution capacity | Fully experienced sponsor with complete in-house capability across every relevant market |
The practical implication: FSP transfers execution capacity to the CRO while keeping governance with the sponsor. When a study runs over, or an inspection happens, the sponsor’s SOPs are the reference standard, and the sponsor’s team is accountable for what went into the eTMF.
When FSP is the right choice
FSP makes sense when the sponsor already has what it needs to run a study strategically, but lacks the bandwidth or regional capacity to staff it operationally.
You have an internal clinical operations structure
There is a sponsor project manager or head of clinical operations who can provide direction, handle escalations, and manage the CRO relationship. They don’t need to be full-time on the study, but they need genuine accountability for it.
Your SOPs and systems are functional
The study runs on your EDC, your eTMF, and your SOP framework. If those are not in place, full-service is the more appropriate choice.
You need regional depth, but you don’t have it in-house
This is the most common trigger for FSP in APAC. A US or European sponsor running a Phase II in Singapore, Thailand, or Malaysia often has strong internal operations capability globally but no on-ground CRA presence in the region. An FSP arrangement with Credevo places experienced local CRAs into the study without transferring project management accountability.
You want to maintain IP and data governance
Because the study team uses the sponsor’s systems throughout the trial, the sponsor retains all data within its infrastructure for the entire study lifecycle. This matters for sponsors sensitive about study data sitting in a CRO’s environment.
When FSP is the wrong choice
The model breaks down in predictable ways, and most failure points are visible before the study starts.
No functioning sponsor-side project manager
The most common failure mode. The sponsor nominates a project manager who lacks the capacity or authority to direct the work. FSP staff then either wait for direction or make decisions outside their remit. The study slows or drifts. This is not a CRO problem: it is a governance gap that no external provider can fill.
SOPs and systems are incomplete or inconsistent
FSP staff work to sponsor SOPs. If you have not clearly structured your eTMF, documented your monitoring visit procedures, or validated your EDC, adding staff creates risk rather than capacity. The staff will ask the sponsor what to do because the sponsor has not yet established the framework they are expected to follow.
Entering a region for the first time
FSP requires that strategic knowledge of the country, the sites, and the regulatory environment sits with the sponsor. If you have no APAC experience, you need a full-service partner who can carry those responsibilities, not a provider executing within a framework you haven’t yet built.
The study is highly complex or novel
First-in-human studies, adaptive designs, or studies with complex biomarker endpoints typically require an integrated CRO team with study design expertise. FSP is an execution model. It is not the right fit when the sponsor also needs advisory capability alongside operational delivery.
What successful FSP relationships look like
When the conditions are right, FSP consistently delivers outcomes that full-service arrangements rarely match. Here is what sponsors report when it works well.
Faster site activation
On-ground FSP staff with established local relationships activate sites faster than remotely managed CRAs. In APAC markets, investigators respond better to CRAs they know personally. A local, embedded presence accelerates the pre-activation conversations that determine how quickly a site is ready to enrol.
Stronger investigator relationships over time
FSP staff are placed for the study duration rather than rotated across a CRO portfolio. Sponsors running multi-cycle programmes in Japan, South Korea, or India find that FSP staff become a genuine relationship asset at key sites, which carries real value in relationship-first markets.
Cleaner accountability and faster issue resolution
When CRAs report to the sponsor project manager directly, accountability is cleaner than in a full-service structure with an intervening CRO project management layer. Issues surface faster. Corrective actions are taken directly.
Meaningful cost savings
Sponsors with functioning internal infrastructure consistently report 20 to 35% savings versus equivalent full-service arrangements in APAC. The savings are real, but they are a consequence of the model working correctly, not a reason to choose it before the preconditions are in place.
The most effective FSP arrangements share three characteristics
The sponsor and FSP provider should establish a defined escalation path from FSP staff to the sponsor project manager and sponsor leadership, conduct monthly operational reviews, and complete a shared onboarding checklist before placing staff.
The diagram below shows how reporting, direction, and escalation flow through a well-structured FSP engagement. Solid arrows show how instructions move downward from the sponsor to sites. Dotted arrows show how reports and escalations travel back up.
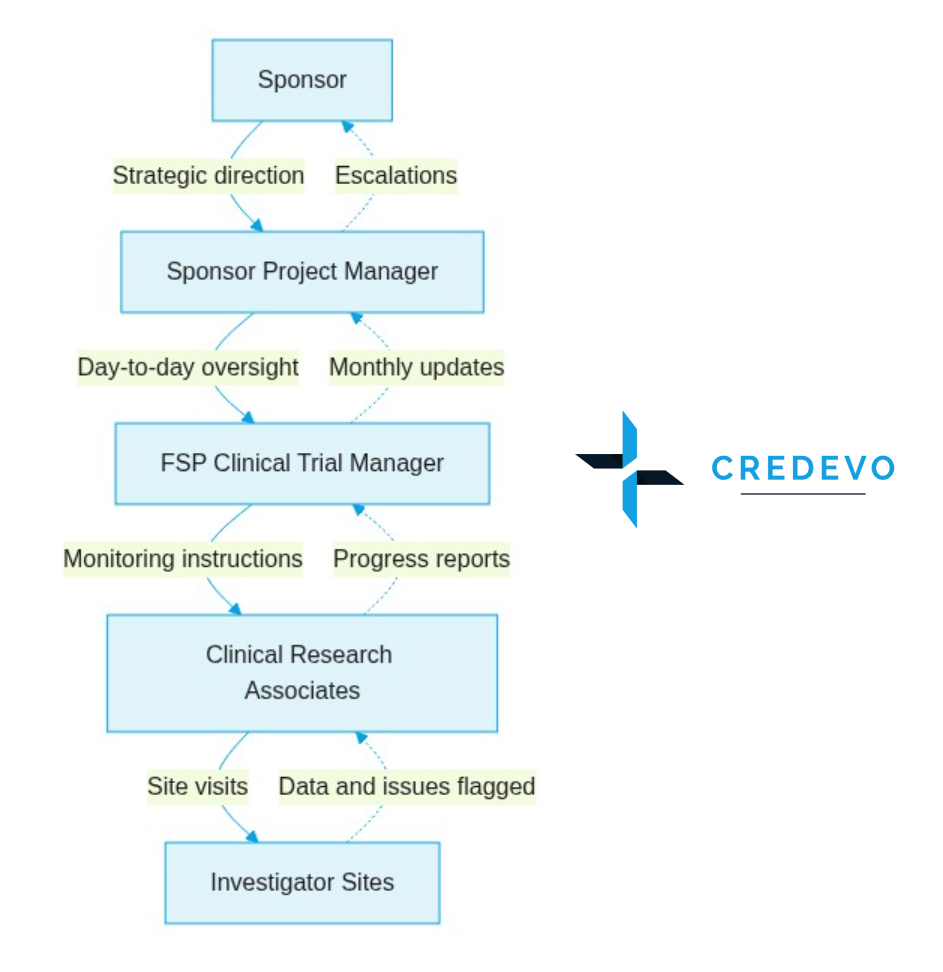
Figure 2: FSP reporting and escalation structure.
Solid arrows: direction of work instructions. Dotted arrows: reporting and escalation path from sites back to the sponsor. A functioning monthly operational review between the sponsor project manager and the FSP clinical trial manager is the single most important governance mechanism in an FSP engagement.
What sponsors get wrong about FSP governance
Accountability doesn’t transfer to the CRO
In a full-service model, the CRO project manager owns the study operationally, and the sponsor holds them accountable for delivery. In FSP, the sponsor owns the study. If a monitoring visit is missed, if eTMF filing falls behind, or if a site relationship deteriorates, those are the sponsor project manager’s problems to resolve. The FSP provider is responsible for the quality of the people it places. The sponsor is responsible for how those people are directed. Sponsors who approach FSP as full-service but cheaper are consistently disappointed.
Onboarding takes longer than expected
FSP staff can’t start until the sponsor delivers SOP training, eTMF access, EDC credentials, and study-specific guidance. This timeline is sponsor-controlled, and in practice, it slips by four to six weeks from contract execution. Building a realistic onboarding plan into a study startup, with a sponsor-side coordinator assigned to it, prevents most of this delay.
The rate card is not the total cost
The FSP fee covers staff time. It does not cover the sponsor project manager, the systems the staff use, training overhead, or inspection readiness activities. Direct FSP-versus-full-service cost comparisons are only accurate when internal sponsor costs are included in both scenarios.
Staff continuity is a shared responsibility
A CRO will backfill departing staff, but backfill takes time and restarts the onboarding process. Sponsors who invest in making the FSP working environment stable (clear direction, responsive project manager, reasonable visit scheduling) retain staff longer and see better site continuity as a result.
FSP in APAC: what’s different
FSP in Asia-Pacific has specific characteristics that sponsors coming from a US or European FSP experience should plan for.
Language and local regulatory knowledge are non-negotiable
CRAs monitoring sites in Japan need to speak Japanese and understand PMDA’s GCP framework. CRAs in India need to be familiar with CDSCO requirements. CRAs in Thailand operate under Thai FDA regulations that differ from those of both. The FSP provider’s ability to place staff with genuine language fluency and local regulatory knowledge, not just English-language competence and general GCP training, is the critical capability to assess.
Site relationship dynamics are different
In Japan, South Korea, and Taiwan, investigator relationships are relationship-first and time-dependent. A CRA new to a site carries less influence than one who has been visiting for several cycles. Ask FSP providers how they manage site relationship continuity when CRA assignments change, and what turnover rates look like by market.
Your systems may need configuration for local requirements
An eTMF structure built for US or European inspections may not map cleanly onto PMDA, CDSCO, or Philippine FDA documentation requirements. This review should happen before FSP staff are placed, not after.
Credevo’s FSP model is available across Singapore, Thailand, Malaysia, India, and Sri Lanka, with on-ground staff embedded in the local clinical trial ecosystem in each market. For context on how FSP has been applied in specific APAC markets, see how the model works in Thailand and India.
What to look for in an FSP provider
Five questions to ask any FSP provider before you commit.
| Question | Why it matters | What a good answer looks like |
|---|---|---|
| What are your CRA turnover rates by market? | High turnover is the strongest predictor of site relationship damage and monitoring quality problems. | Specific rates by country, not a vague “low turnover” claim. |
| Are your CRAs locally based or regionally managed? | A provider managing APAC from a central hub differs from one with staff embedded in each country. | Named local trial managers in each country, not a regional office overseeing all markets. |
| How do you onboard staff to sponsor SOPs? | A provider without a formal SOP onboarding process will improvise, which means your CRAs will too. | Documented onboarding checklist, defined timeline, named coordinator. |
| Has your team supported regulatory inspections in these markets? | Inspection experience affects how staff document and how they manage site staff in ways that only become visible during an inspection. | Named markets with specific inspection experience (PMDA, CDSCO, Thai FDA). |
| What is your escalation structure for issues the CRA cannot resolve? | In FSP, the CRO is not the decision-maker on protocol or site issues, but operational problems still need a clear escalation path. | What is your escalation structure for issues that the CRA cannot resolve? |
Conclusion
The FSP model is not a shortcut to cheaper trials. It is a structure that amplifies what a well-organised sponsor already has: adding regional execution depth, maintaining data control, and building site relationship continuity that full-service rotations often don’t. Sponsors who choose it for the right reasons and build the internal conditions it requires consistently report some of the strongest operational outcomes in APAC clinical research. The governance sits with you. The execution strength comes from the provider. When both sides of that equation are functioning, the model works well.
Are You Planning an APAC Trial and Weighing the FSP Model?
If you want to assess whether your current operations setup is ready for FSP, or whether a full-service or hybrid arrangement better fits your programme, Credevo can review the structure with you before you commit. Talk to the team at credevo.com/contact.
Glossary
- APAC: Asia-Pacific.
- CRA (Clinical Research Associate): The on-site monitor who visits investigator sites to verify data accuracy and protocol compliance.
- CDSCO: Central Drugs Standard Control Organisation. India’s national drug and medical device regulator.
- CRO (Contract Research Organisation): A company that provides clinical trial services to sponsors on an outsourced basis.
- CTMS (Clinical Trial Management System): Software used to manage and track the operational details of a clinical trial.
- EDC (Electronic Data Capture): The software system into which clinical trial data is entered at the site.
- eTMF (Electronic Trial Master File): The system that stores all essential documents required to verify trial conduct and regulatory compliance.
- FSP (Functional Service Provider): A CRO engagement model where the provider supplies staff to work within the sponsor’s own governance structure, SOPs, and systems.
- GCP (Good Clinical Practice): The international quality standard for the design, conduct, and reporting of clinical trials. Set by the ICH.
- ICH (International Council for Harmonisation): The body that sets GCP and other pharmaceutical development standards used globally.
- IND (Investigational New Drug): A US FDA application that permits a new drug to be studied in human subjects.
- IP (Intellectual Property): Proprietary information such as compound data, formulations, and study results.
- PMDA: Pharmaceuticals and Medical Devices Agency. Japan’s national regulator for drugs, medical devices, and biologics.
- SOP (Standard Operating Procedure): A written instruction that defines exactly how a task must be performed to meet quality and regulatory standards.
- Thai FDA: Thailand Food and Drug Administration. Thailand’s national regulator for medicines, food, and medical devices.
Frequently asked questions
Q: What is the difference between FSP and CRO staff augmentation?
In staff augmentation, individual contractors are placed directly with the sponsor on a time-and-materials basis, often without a CRO layer. In FSP, the provider retains employer accountability for the staff, manages HR and backfill, and provides oversight of placed staff performance. The sponsor directs the work; the FSP provider is responsible for the quality of the people doing it. FSP typically involves more structure and more provider accountability than a pure staff augmentation arrangement.
Q: Can a sponsor use FSP for only part of a study, then transition to full-service or bring work in-house?
Yes, though transitions add risk. The eTMF structure, site relationships, and data documentation history all need to transfer cleanly. If the sponsor’s systems are the record of authority throughout, a transition to a different staffing model is manageable. If the sponsor is also changing systems mid-study, the complexity multiplies. Plan any transition at a natural break point: ideally between phases or at a scheduled database snapshot.
Q: Is FSP appropriate for sponsors running their first clinical trial?
Generally not. The FSP model requires a functioning sponsor-side infrastructure: SOPs, systems, a capable project manager, and operational experience. A first-time sponsor does not yet have that. Full-service with a CRO that includes advisory capability is more appropriate until the sponsor has built the internal infrastructure to support the FSP model.
Q: How does FSP affect the sponsor’s ICH E6(R3) compliance obligations?
Under ICH E6(R3), which took effect in 2025, the sponsor’s obligation to maintain quality oversight of delegated activities is explicit. In an FSP arrangement, the sponsor delegates operational functions but retains regulatory accountability. The sponsor must maintain documented delegation, training records, oversight visit schedules, and a clear process for handling deviations. The FSP provider’s staff working under sponsor SOPs does not transfer the sponsor’s compliance obligations.
Q: What is a reasonable FSP staffing ratio for an APAC Phase II oncology study running across three countries?
A Phase II oncology study across three APAC markets typically requires one clinical trial manager per country (or one manager overseeing two smaller sites), plus CRAs at roughly one per two to three active sites, depending on visit frequency and protocol complexity. Data management may be handled separately. Credevo can provide a staffing estimate based on the specific protocol and country plan.