Optimizing Clinical Trials in Triple-Negative Breast Cancer: Biomarker Integration, Recruitment Strategies, and Investigator Engagement
Key Takeaways from the Article
- Early investigator engagement improves protocol feasibility, reduces amendments, accelerates study startup timelines, and strengthens recruitment performance in TNBC clinical trials.
- Triple-Negative Breast Cancer (TNBC) is an aggressive and highly heterogeneous subtype of breast cancer with limited treatment options and significant unmet clinical needs.
- Biomarker-driven strategies involving PD-L1, BRCA mutations, HRD, and next-generation sequencing are reshaping precision medicine approaches in TNBC drug development.
- Patient recruitment remains a major challenge due to strict eligibility criteria, biomarker requirements, competition among trials, and patient access barriers.
- Technology-enabled clinical trial operations, decentralized trial models, AI-driven analytics, and CRO partnerships are becoming essential for efficient oncology trial execution.
Triple-Negative Breast Cancer (TNBC) remains one of the most aggressive and complex forms of metastatic breast cancer, presenting major challenges for sponsors, investigators, and CROs in oncology drug development. As biomarker-driven therapies, immuno-oncology approaches, and precision medicine strategies rapidly evolve, early investigator engagement has become essential for successful clinical trial execution.
Strategic collaboration during protocol development, feasibility assessment, and site selection can improve recruitment performance, enhance protocol efficiency, reduce startup delays, and optimize patient-centric trial outcomes.
This article highlights the evolving TNBC clinical landscape, operational challenges, and innovative CRO-led strategies that support faster, smarter, and more efficient oncology trial delivery.
1. Introduction to Metastatic Breast Cancer (MBC) and Triple-Negative Breast Cancer (TNBC)
Metastatic Breast Cancer (MBC) refers to breast cancer that has spread beyond the breast and regional lymph nodes to distant organs such as the lungs, liver, bones, or brain. Among all breast cancer subtypes, Triple-Negative Breast Cancer (TNBC) represents approximately 10–15% of cases and is characterized by the absence of estrogen receptors (ER), progesterone receptors (PR), and HER2 expression.
Due to the lack of targeted hormonal therapies, TNBC is often associated with aggressive tumor biology, rapid disease progression, higher recurrence rates, and poorer survival outcomes compared to other breast cancer subtypes. Although recent advances in immunotherapy, antibody-drug conjugates (ADCs), and biomarker-driven therapies have transformed the treatment landscape, substantial unmet medical needs still remain. As a result, TNBC continues to be a major focus area in oncology clinical research and drug development.
Subtypes of Metastatic Breast Cancer (MBC)
The table outlines the major subtypes of Metastatic Breast Cancer (MBC), including TNBC, along with their key characteristics and treatment approaches.
| Classification / Type | Receptor Status | Key Characteristics | Common Treatment Approaches |
| Hormone Receptor-Positive (HR+)/HER2-Negative | HER+ and/or PR+, HER2- | Most common subtype; slower growing compared to TNBC | Endocrine therapy, CDK4/6 inhibitors, targeted therapy |
| HER2-Positive Breast Cancer | HER2+ may be ER/PR positive or negative | HER2+ may be ER/PR positive or negative | HER2-targeted therapy, chemotherapy, ADCs |
| Triple-Negative Breast Cancer (TNBC) | ER-, PR-, HER2- | Highly aggressive, higher recurrence risk, limited targeted options | Chemotherapy, immunotherapy, ADCs, PARP inhibitors |
| Luminal A | ER+/PR+, HER2-, low Ki-67 | Slow-growing, better prognosis | Hormonal therapy |
| Luminal B | ER+, may be HER2+, higher Ki-67 | Faster growing than Luminal A | Hormonal therapy, chemotherapy, targeted therapy |
| Basal-like Breast Cancer | Usually TNBC phenotype | Aggressive molecular subtype associated with BRCA mutations | Chemotherapy, PARP inhibitors, immunotherapy |
| BRCA-Mutated Metastatic Breast Cancer | Can occur in multiple subtypes | Associated with DNA repair defects | PARP inhibitors, platinum-based chemotherapy |
| PD-L1 Positive TNBC | TNBC with PD-L1 biomarker expression | Eligible for immunotherapy-based treatment strategies | Immune checkpoint inhibitors + chemotherapy |
2. Disease burden and unmet clinical needs in TNBC
The global burden of TNBC continues to rise, particularly among younger women, patients with BRCA mutations, and certain ethnic populations. TNBC is associated with shorter progression-free survival (PFS), limited treatment options, and increased risk of visceral metastases. Despite improvements in systemic therapies, many patients experience relapse within the first few years following diagnosis. Additionally, treatment resistance remains a major obstacle in metastatic TNBC management. The lack of durable therapeutic responses highlights the urgent need for innovative treatment strategies and better patient stratification approaches.
TNBC clinical trials must address not only efficacy, but also quality of life, treatment tolerability, and access to advanced therapies. These unmet clinical needs continue to drive intensive oncology research and global clinical trial activity.
3. Molecular landscape and emerging biomarkers in TNBC
The molecular complexity of TNBC has significantly evolved over the past decade. Previously considered a single disease entity, TNBC is now recognized as a highly heterogeneous disease with multiple molecular subtypes.
Biomarkers such as PD-L1, BRCA1/2 mutations, tumor mutational burden (TMB), homologous recombination deficiency (HRD), and androgen receptor expression are increasingly shaping treatment decisions and clinical trial design.
The growing use of next-generation sequencing (NGS) and precision medicine has helped identify new therapeutic targets and improve patient selection. Biomarker-driven trial designs are becoming essential in TNBC studies to improve response rates, reduce trial failure risk, and support personalized treatment strategies. As translational research advances, molecular profiling will continue to play a central role in future TNBC clinical development.
4. Current and emerging treatment landscape in TNBC
The treatment landscape for TNBC has evolved rapidly with the introduction of immunotherapies, PARP inhibitors, antibody-drug conjugates, and targeted therapies. Historically, chemotherapy remained the primary treatment option for TNBC patients due to the absence of actionable receptors. However, recent approvals of immune checkpoint inhibitors and targeted agents have improved treatment outcomes in selected patient populations.
Emerging therapies targeting Trop-2, PI3K/AKT pathways, and DNA damage repair mechanisms are also showing promising results in ongoing clinical trials. Combination therapies involving chemotherapy, immunotherapy, and targeted agents are being explored to improve survival outcomes and overcome resistance. Despite these advancements, identifying the right patient population and optimizing sequencing strategies remain critical challenges in TNBC therapeutic development.
5. Clinical trial landscape and evolving study designs in Metastatic TNBC
The clinical trial landscape in metastatic TNBC is highly competitive and rapidly evolving. Sponsors are increasingly using adaptive designs, basket studies, umbrella trials, and biomarker-enriched protocols to accelerate development and improve trial efficiency. Global oncology pipelines for TNBC continue to expand, leading to increased competition for eligible patients and experienced investigative sites. Protocol complexity, stringent eligibility criteria, and operational burdens often contribute to enrollment delays and site fatigue.
To address these challenges, sponsors are integrating decentralized trial elements, digital technologies, and patient-centric methodologies into oncology studies. Innovative trial designs and operational flexibility are essential to enable faster recruitment, better retention, and improved data quality in TNBC clinical research.
6. Importance of early investigator engagement in TNBC trial design
Early investigator engagement plays a critical role in improving the feasibility, efficiency, and scientific quality of TNBC clinical trials. Investigators provide valuable insights into patient populations, local standards of care, competing studies, protocol practicality, and recruitment feasibility. Early investigator engagement helps identify operational barriers during protocol development, reducing costly amendments and delays later in the trial. Investigator feedback can also improve inclusion and exclusion criteria, optimize visit schedules, and enhance patient-centric trial design.
In competitive oncology studies, early collaboration with key opinion leaders (KOLs) and experienced investigators strengthens site commitment and enrollment performance. As oncology trials become increasingly complex, strategic investigator engagement has become a critical differentiator for successful clinical development.
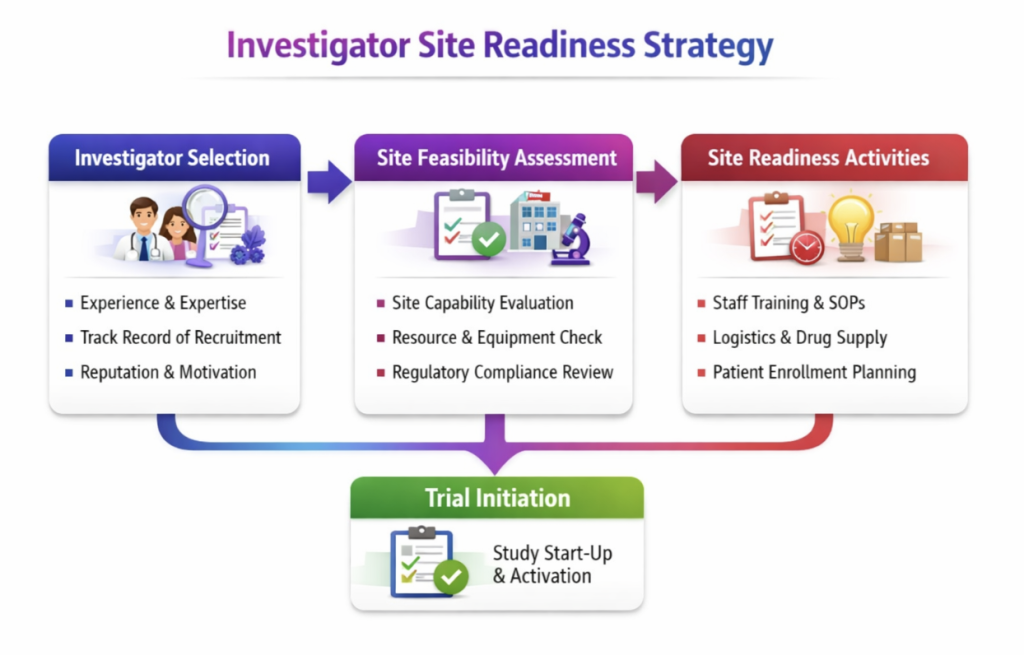
7. Investigator selection, site feasibility, and site readiness strategies
Selecting the right investigators and ensuring site readiness are essential for successful TNBC trial execution. High-performing oncology sites should have strong patient access, experienced research teams, biomarker testing capability, and infrastructure for complex study procedures.
Sponsors and CROs must conduct feasibility assessments to evaluate site capabilities, competing trial burden, patient demographics, and past enrollment performance. Early site engagement, training programs, and proactive communication strategies can improve site preparedness and reduce startup delays.
Centralized support models, technology-enabled feasibility tools, and real-world data analytics are increasingly used to identify optimal investigative sites. A well-planned site readiness strategy can significantly enhance enrollment efficiency and study execution quality.
8. Patient recruitment and enrollment challenges in TNBC clinical trials
Patient recruitment remains one of the most significant challenges in TNBC clinical trials. The aggressive nature of the disease, strict eligibility criteria, biomarker requirements, and limited patient pools often slow enrollment timelines. In addition, increasing competition among oncology studies can make patient retention and investigator engagement more difficult.
Geographic disparities, socioeconomic barriers, and limited awareness of clinical trials also contribute to recruitment challenges. Many patients face logistical burdens related to travel, treatment schedules, and frequent study visits, which may impact participation and compliance. To address these issues, sponsors must adopt patient-centric recruitment strategies focused on accessibility, diversity, education, and engagement throughout the clinical trial journey.
9. Strategies to improve patient recruitment, diversity, and retention
Improving patient recruitment and retention in TNBC trials requires a comprehensive and patient-focused approach. Sponsors and CROs are increasingly using digital recruitment, patient advocacy partnerships, social media, and community outreach to increase trial awareness. Diversity and inclusion initiatives are also becoming critical to ensure equitable representation across racial, ethnic, and underserved patient populations.
Simplifying procedures, reducing patient burden, offering travel support, and using decentralized trial elements can improve retention and trial experience. In addition, transparent communication and strong site-patient relationships help build trust and encourage long-term participation. Successful recruitment strategies must balance scientific rigor with patient accessibility and operational flexibility.
10. Role of CROs and strategic partnerships in accelerating TNBC clinical development
Contract Research Organizations (CROs) play an increasingly important role in accelerating TNBC clinical development by providing operational expertise, global site networks, regulatory support, and technology-driven solutions. CROs help sponsors streamline study startup activities, optimize feasibility assessments, manage site relationships, and improve recruitment strategies.
Strategic collaborations between sponsors, CROs, academic institutions, and patient advocacy groups can enhance study execution and accelerate innovation in oncology research. In highly competitive therapeutic areas such as TNBC, CROs also support risk mitigation, data management, and decentralized trial implementation. As clinical trial complexity continues to grow, integrated partnerships and collaborative development models are becoming essential for successful oncology trial delivery.
11. Technology and innovation in oncology clinical trial operations
Technology is transforming oncology trials through AI, electronic data capture (EDC), remote monitoring, wearables, and digital patient engagement platforms. Advanced analytics and predictive modeling are increasingly being used to improve feasibility assessments, identify recruitment risks, and optimize operational planning.
Moreover, decentralized clinical trial (DCT) models and hybrid approaches are helping reduce patient burden while expanding access to broader patient populations. In addition, real-world evidence (RWE), electronic health records (EHRs), and digital biomarkers are supporting more efficient trial execution and data collection.
As innovation continues to reshape clinical research, technology-driven operational strategies will become increasingly important in future TNBC studies.12. Regulatory considerations and market access landscape
The regulatory landscape for TNBC therapies continues to evolve as agencies prioritize accelerated approvals for innovative oncology treatments addressing high unmet medical needs. Regulatory authorities increasingly encourage biomarker-driven development, adaptive trial designs, and patient-focused endpoints to support faster therapeutic innovation.
Sponsors must also navigate evolving requirements related to companion diagnostics, safety monitoring, and global regulatory harmonization. Beyond regulatory approval, market access and reimbursement considerations are becoming increasingly important in oncology commercialization strategies. Demonstrating clinical value, real-world effectiveness, and health-economic benefits is essential for successful market adoption. Early integration of regulatory and market access planning can significantly improve overall development efficiency and commercialization success.
13. Future perspectives in TNBC clinical research and trial execution
The future of TNBC clinical research will likely be shaped by precision oncology, personalized medicine, AI-driven analytics, and increasingly patient-centric trial models. Furthermore, emerging therapies such as cell therapies, bispecific antibodies, novel ADCs, and combination immunotherapies are expected to transform treatment paradigms.
Additionally, decentralized trial technologies and digital health innovations will continue improving operational efficiency and patient accessibility. Moreover, investigator collaboration, global partnerships, and integrated data ecosystems will play a critical role in accelerating drug development timelines. As scientific understanding of TNBC continues to evolve, future clinical trials must remain adaptive, collaborative, and innovation-focused to address ongoing unmet needs.
Conclusion
Triple-Negative Breast Cancer (TNBC) remains one of the most challenging areas in oncology drug development due to its aggressive biology, molecular heterogeneity, and evolving treatment landscape. As clinical research advances, early investigator engagement has become increasingly important for improving protocol feasibility, enhancing site readiness, optimizing patient recruitment, and accelerating study execution.
Industry experts continue to emphasize that scientific innovation and operational excellence must work together to improve outcomes in TNBC clinical research. Biomarker-driven development, adaptive trial designs, patient-centric operational models, and decentralized technologies are reshaping the future of oncology trials.
In addition, growing focus on diversity, inclusion, and equitable trial access highlights the need for stronger collaboration among sponsors, investigators, CROs, regulators, and patient communities. By integrating precision medicine strategies, innovative technologies, and collaborative clinical development approaches, the oncology industry can improve trial efficiency and ultimately deliver more effective therapies to patients with TNBC.
Need Support for TNBC Clinical Trials and Oncology Research?
Triple-Negative Breast Cancer (TNBC) clinical trials present significant challenges in oncology drug development, including patient recruitment, biomarker-driven study design, investigator engagement, and the complexities of global trial execution. If you are facing any of these challenges or require support in the clinical development of metastatic breast cancer therapies, please fill out the form below to connect with our team and discuss how we may be able to assist.